What 25 Years of Coding Taught Me About G2211, Modifier 25, and Dual Visits



A 25-year coding and auditing veteran explains how Arintra autonomously handles G2211, modifier 25, dual visits, and new vs. established patient logic inside Athena capturing compliant revenue without manual intervention.
By Susan Oprean, VP of Revenue Cycle at Arintra
In a recent webinar, I discussed how Arintra handles complex coding workflows autonomously with our CEO, Nitesh Shroff. We focused on some of the scenarios that typically require manual review, such as G2211, dual visits, modifier 25, and new vs. established patients. These are areas where I see a lot of confusion and, frankly, a lot of revenue left on the table.
For context, I've been in medical coding and auditing for over 25 years (at this point, I've stopped counting). I'm a certified coder and auditor. The workflows I'm describing below reflect both compliance best practices and the configurability our clients need.
Nitesh opened the webinar by talking about how Arintra works directly inside Athena, and I want to start there because the Athena integration is central to how all of this works in practice.
How Arintra Works Inside Athena
Arintra has been on the Athena marketplace for four years now. We understand the ecosystem, the APIs, and how Athena workflows function in practice. That experience matters because we're not asking your team to step outside of Athena or learn a new system. The coding automation happens entirely inside Athena.
Let me give a quick rundown of how this works. Arintra pulls the clinical documentation from a chart, including HPI, past medical history, the assessment, plan, and medications, and runs it through our coding engine. The engine has multiple layers:
- Clinical understanding. The AI interprets all aspects of the documentation, such as whether diabetes is stable, whether back pain is acute or chronic, whether surgery was done on the left knee or the right knee, or whether a medication was changed.
- Compliance layers. The engine applies state-specific MAC guidelines, national CMS guidelines, CCI edits, LCD and NCD edits, ICD-10 guidelines, including Excludes1 edits, and payer configurations.
- Code generation. The final set of codes includes E/M, ICD-10 linked to specific CPT codes, HCC codes, modifiers, and units.
Arintra’s coding engine sits between the providers and the coders. The moment a provider completes a note, we pull the chart data, generate the codes, and write them back into Athena. Around 86% of charts are coded automatically. The other 14% go into a hold queue for the organization’s coders in Athena with a specific action item: missing documentation, a conflicting diagnosis, or an unmet payer requirement. There are no workflow changes for providers.
Every code Arintra generates is fully explainable. You can click on any code to see the clinical documentation that supports it, and all codes are auditable through the Arintra Codex app right inside Athena.
G2211: Visit Complexity Add-On
Let’s start with a fun one (at least for a longtime coder). G2211 is an add-on code for E/M services, used when a provider is managing a patient's ongoing care, typically for chronic conditions. There are specific rules for when it applies and when it doesn't, and a lot of organizations are still figuring out how to code it consistently.
Our out-of-the-box logic involves a conservative approach that looks like this:
- Established patients only: G2211 can technically apply to new patients, but an established patient is a stronger signal that there's a longitudinal relationship between provider and patient.
- Chronic conditions managed: It can apply to acute conditions, but it's harder to identify how long the provider is going to be taking care of that patient in acute cases.
- Medicare and Medicare Advantage: This is configurable based on each client's payer mix and needs.
- Modifier 25 rules: About a year or two ago, the Centers for Medicare & Medicaid Services (CMS) clarified that G2211 can be used with modifier 25 under certain circumstances. If modifier 25 is being added for vaccine administration (90471) or a CMS-covered preventive service like an annual wellness visit, G2211 is allowed.
We always link G2211 to chronic conditions in the documentation. But every piece of this logic is configurable by organization, including the way payer rules are set up.
Dual Visits: Proving Separate Significant Work
Dual visits happen when a patient comes in for an annual wellness visit (Medicare G0402, G0438, or G0439 codes) or a preventive service (your 993XX codes) and the provider also addresses a separate problem. To bill the additional E/M, you have to demonstrate separate significant work.
We've broken this into three pathways:
1. Acute illness: While the patient is there for preventive care, is there an acute problem being addressed? Maybe the patient mentions sinusitis, complains about a rash, or is experiencing some form of pain that needs attention. We look for:
- An acute condition addressed
- Evaluation of that condition
- Management is required: Is there a referral? Follow-up labs? Prescription drug management?
2. Unstable chronic condition: If a patient comes in for their annual well visit and they have uncontrolled diabetes or hypertension, for example, the provider has to address it. We want to make sure providers are compensated for that extra service. So we look for:
- Evaluation of the unstable condition
- Management changes, for example: adjusting medication or dosage, ordering labs to check A1C or glucose, or lipid panels
3. Stable chronic condition: This is more of a gray area. Let’s say a patient comes in for a 6-month checkup for a stable chronic condition. Extra work like diagnostics, lab work, or additional testing that falls outside the preventive or annual well visit qualifies as separate significant work. We look at:
- Signs and symptoms the patient is showing
- Review of prior results (checking the patient's blood pressure diary, looking over last test results)
- Ongoing management (continue current medication, order follow-up labs, referral for other care)
Some clients are very conservative and don't bill the additional E/M for stable chronic conditions. Others will bill it if two or more stable conditions are being managed. We can also configure requirements around patient notification, such as a note in the record that the patient was informed they might receive an additional charge. All of this is configurable in Arintra's engine rules.
Modifier 25: When It Applies (and When It Doesn't)
Modifier 25 is highly scrutinized and overuse may lead to audits. So we look carefully for separate significant work before applying it.
The logic follows the same principles as dual visits. If you're doing a dual visit, there has to be additional work outside of what you're already getting paid for with the annual well visit or preventive service. The same logic applies to procedures and injections.
Here are a few examples:
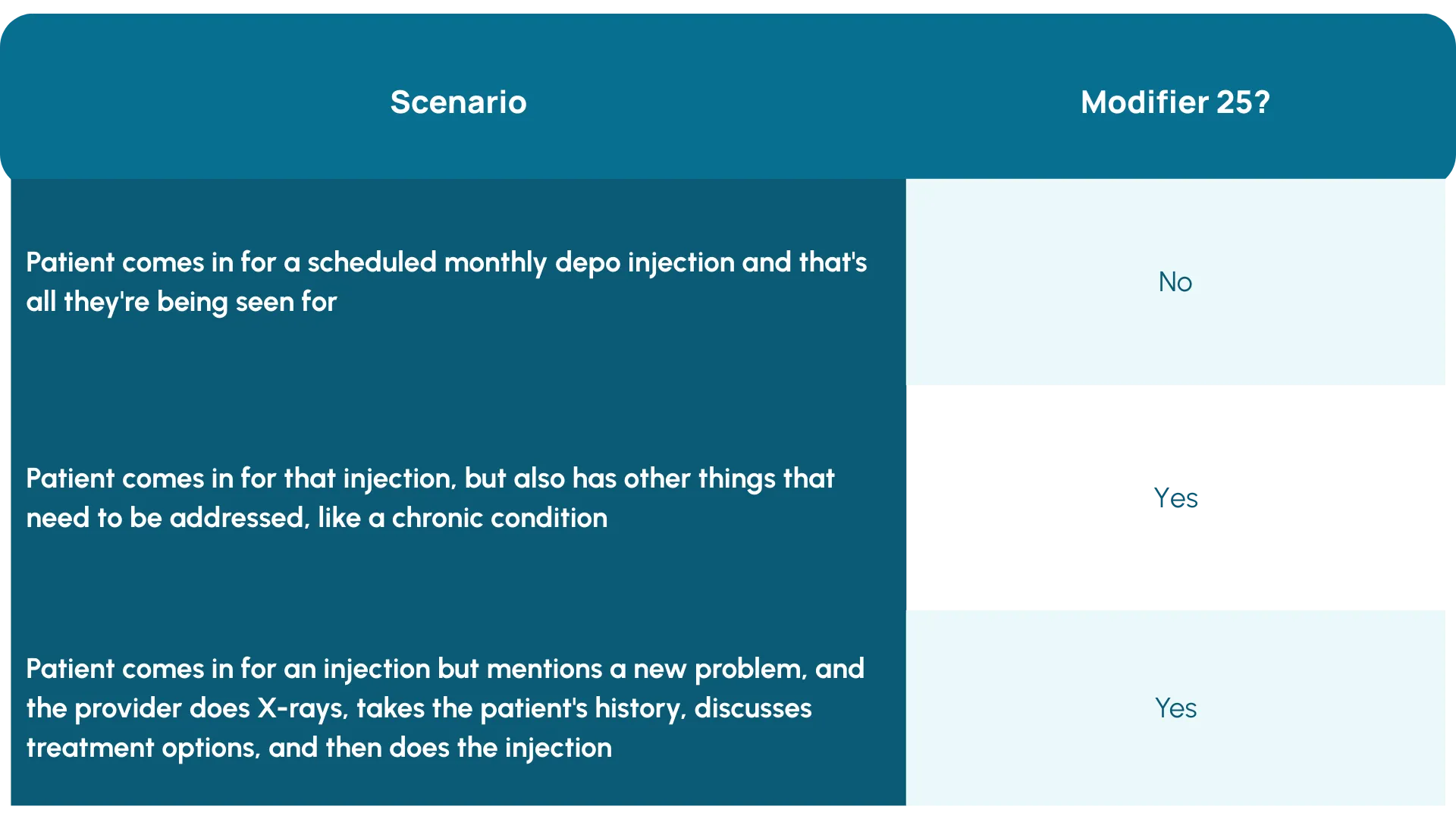
The key is whether the work falls outside what's already covered in the procedure's pre-op and post-op. If it does, modifier 25 applies. We also make sure diagnosis codes are linked appropriately so that the procedure gets the diagnoses for what it's treating, and the E/M gets the diagnoses for the separate significant work.
New vs. Established: More Complex Than It Looks
We find that a lot of electronic medical records cannot handle the new versus established distinction appropriately, mainly in relation to the mid-levels. Nurse practitioners and PAs have the same taxonomy (a PA is a PA and an NP is an NP), which creates problems.
We use multiple layers to get this right:
- NPI. Has the patient seen a provider with the same NPI within the last three years? If yes, it's not new.
- Taxonomy. Has the patient seen a provider in the group with the same taxonomy? If yes, it's not new.
- Specialty. This is the department they're working in, not the taxonomy specialty. If an NP is working in primary care, they're going to have a specialty of primary care and be compared against the MDs also working in primary care. So if a patient sees an MD and then comes back to see an NP in primary care, the output is established.
We also handle state-specific variations. Some states now allow NPs to bill as new when working in different specialties, so we've built workflows for that. A patient who saw an NP in primary care and now sees an NP in cardiology? That's new for cardiology.
If a provider practices across multiple specialties with different payer rules, we list them twice in our dictionary and apply the appropriate business rules per payer.
What Else We Handle
Beyond these four workflows, Arintra handles a wide range of complex scenarios inside Athena, including:
- TCM workflows
- Prolonged visits
- Telehealth
- Nurse visits and after-hours visits
- Screeners (PHQ-9, GAD-7, ADHD, lung cancer, and others)
- Cat II quality codes
- HCC combination codes
- Vaxcare and vaccine workflows
- Z-code sequencing
- Social determinants of health
Every code we generate includes a full explanation of the clinical documentation that supports it, viewable directly in Athena. Coding is complicated, but it doesn’t have to be painful. That’s the whole point of building logic that handles these workflows automatically.
Organizations using Arintra see an average 5.1% revenue uplift, with some reporting higher depending on specialty mix and baseline accuracy. Want to explore what this looks like for your organization? We'd love to hear from you - hello@arintra.com
Explore More Resources

Is Your Health System Ready for Autonomous Medical Coding? Five Questions to Ask

"Arintra is Doing the Heavy Lifting" Mercyhealth Transforms a Coding Capacity Challenge into Revenue Integrity at Scale

Med First Finds Its ‘Easy Button’ With Arintra: Over 6% Revenue Uplift, Stronger Compliance, and Reduced Provider Burden in One Solution

Mercyhealth boosts revenue by 5% and cuts aging days by over 50% while supporting accelerated growth

The Hidden Power of Coding in Transforming Revenue Cycle Management

Arintra Receives A+* Partnership Rating in KLAS Emerging Company Spotlight Report
Arintra’s Fully Automated Medical Coding Solution Now Available in Epic Toolbox

Mercyhealth Transforms Revenue Cycle Management With Arintra's Autonomous Coding Solution

Still on the fence about autonomous medical coding? Here’s what you’re missing
