What Is Clinical Documentation Improvement? A Closer Look at CDI for Outpatient Care


Clinical documentation improvement (CDI) ensures accurate coding, reduces denials, and improves revenue by capturing complete patient care details.
Ask any coder what frustrates them, and you'll most likely hear some version of this: "I can only code what's documented in the patient’s chart." Clinical documentation that’s vague or missing specificity means that coders have to assign lower-level codes, even when the provider clearly delivered more complex care. The result is that organizations collect less than the care was worth.
That's what clinical documentation improvement (CDI) is designed to address. So what is clinical documentation improvement, exactly? It’s a structured way of ensuring that patient charts reflect the full picture of the care that was delivered, so that coders, billers, and compliance teams all have what they need to do their jobs.
If the term CDI carries some baggage at your organization, it’s understandable. The concept of more accurate, complete documentation is hard to argue with, but historically, getting there has involved significant challenges. CDI can be expensive, create more burden for physicians, and entail layers of administrative overhead that strain already stretched teams. Traditional CDI is often slow, costly, and frustrating for physicians who feel like they’re being nagged about paperwork on top of everything else.
That reality is worth acknowledging upfront, because it’s also what makes newer approaches to documentation improvement so interesting.
CDI in Healthcare Explained: Role in Coding, Compliance & Revenue Cycle
During a patient encounter, providers are documenting with clinical care in mind, not coding. Clinical documentation improvement involves reviewing patient charts to ensure they also capture what coders need, such as:
- Specific diagnoses with clinical detail (type, severity, status)
- Procedures performed during the encounter
- Clinical reasoning behind treatment decisions
- Enough specificity to assign accurate codes
CDI in healthcare connects clinical care and the revenue cycle. Providers should be focusing on patients, while coders later translate that care into standardized codes. CDI healthcare teams sit between those groups, reviewing charts, flagging ambiguities, and issuing physician queries to clarify the record before coding begins.
That's how it's supposed to work anyway. In practice, especially in outpatient care, that’s not what tends to happen. Encounter volumes are enormous, and there aren't enough professional coders to review every chart.
In many ambulatory settings, providers end up coding their own encounters, selecting codes during or after the visit without any CDI or coding oversight. The documentation that supports those codes often goes unreviewed, which means gaps that affect reimbursement and compliance can persist for months or longer without anyone noticing.
Why CDI Matters: Impact on Revenue, Coding Accuracy & Financial Performance
The financial consequences of weak documentation hit organizations and providers at the same time, though in different ways.
How Documentation Affects Coding Accuracy & Reimbursement
At the organizational level, coding accuracy depends entirely on what's in the record. A provider who documents "diabetes" without specifying type, control status, or complications forces the coder to select a less specific ICD-10 code.
That omission can reduce reimbursement and, in risk-adjusted models, affect capitation payments for the entire year.
Reducing Claim Denials with Better Clinical Documentation
Denials trace back to documentation more often than most people realize. A recent survey by the American Hospital Association found that roughly 15% of claims face initial denial, and incomplete documentation drives a large share of those rejections. Each reworked denial costs between $25 and $181 and delays payment by weeks.
Strong clinical documentation integrity also protects organizations during healthcare coding and compliance audits, helping to ensure that records hold up under payer scrutiny.
Impact of CDI on Physicians: Workload, Compensation & Documentation Burden
There's another layer to this conversation. Documentation gaps affect providers personally. Roughly 70% of physician compensation ties directly to work relative value units (wRVUs).
In cases where provider documentation doesn't support the right codes, physicians aren't compensated for the care they deliver. Most providers don't even realize this is happening because nobody has connected their charting habits to the financial impact on their own pay.
What all of this boils down to is that CDI and revenue cycle management are inseparable. Documentation quality determines coding accuracy, which determines whether organizations and providers collect what they've earned.
Challenges in CDI: Administrative Burden, Variability & Coding Complexity
If documentation improvement were straightforward, every health system would already have it figured out. The reality is messier.
Medscape's 2024 physician survey suggests that providers spend an average of 15.5 hours per week on administrative tasks. Adding documentation requirements creates real friction, especially when providers feel like they're charting for coders rather than for patients.
Documentation variability is a genuine challenge for CDI. Two physicians treating the same condition may document it in completely different ways, one with granular specificity and the other with shorthand that coders struggle to interpret. Multiply that across hundreds of providers, and you can see the complexity of this issue.
The move to ICD-10, which expanded the diagnosis code set from roughly 13,000 to around 70,000 codes, raised the bar even more for documentation specificity.
CDI in Outpatient Care: Scale, Volume & Unique Challenges
Most CDI programs were built for inpatient care, where individual claims carry higher dollar values and concurrent chart review makes economic sense. You can assign a CDI specialist to a chart before it goes to coding, because the reimbursement justifies the investment.
Outpatient care doesn't work that way. Encounter volumes dwarf those in inpatient care, the per-claim value is lower, and margins can't absorb the cost of reviewing every encounter manually. And yet the need is just as real. The financial impact accumulates differently, not through a few high-dollar claims, but across thousands of encounters where small documentation gaps add up to significant uncaptured revenue.
Until recently, there wasn't a practical way to address this at scale.
AI in Clinical Documentation Improvement: Automation, Insights & Coding Accuracy
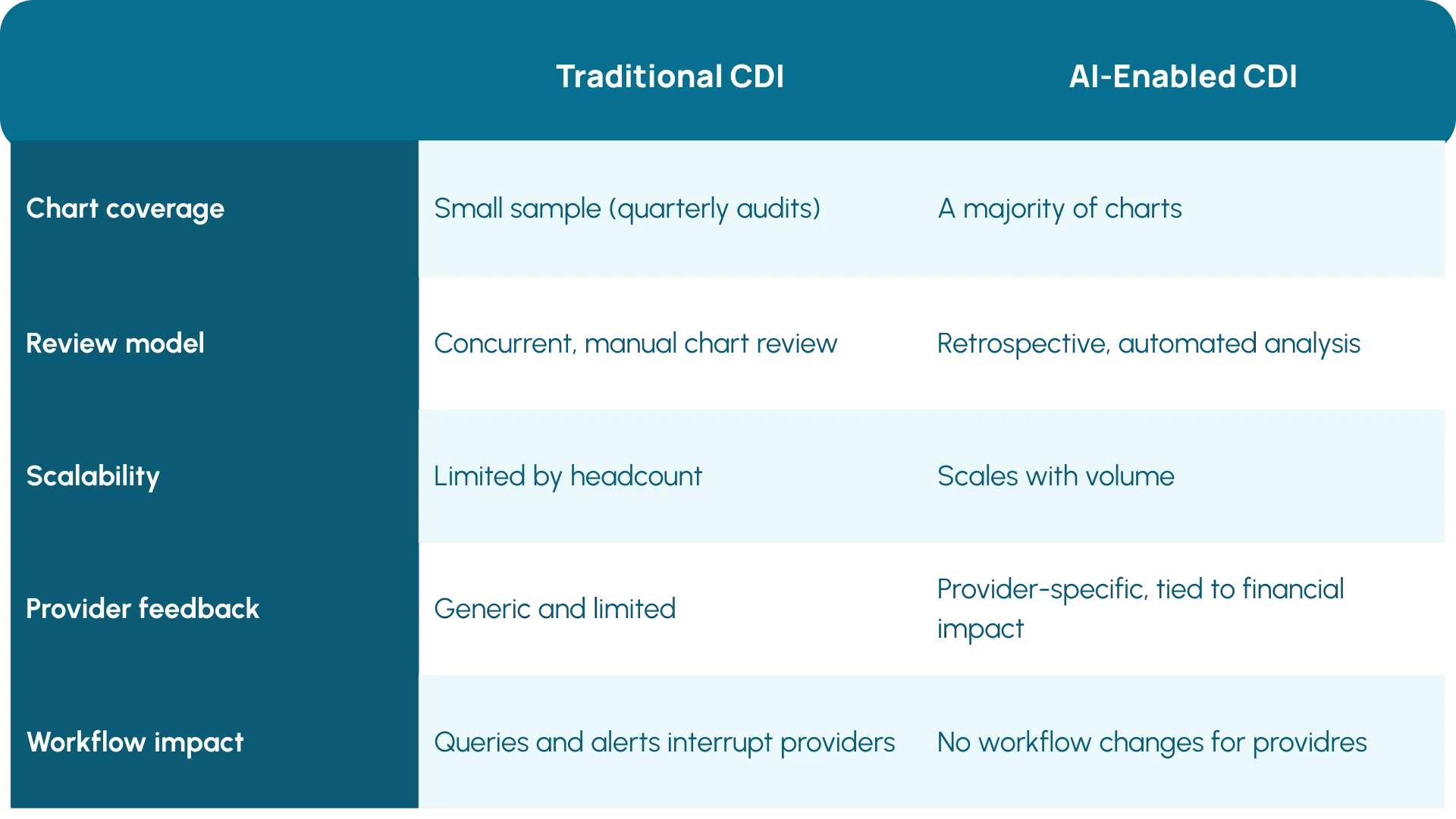
Something worth paying attention to is what happens when you pair CDI with AI-powered autonomous coding platforms. The best platforms process the majority of charts, so they build a detailed picture of how each provider documents. CDI teams can use that data to have very specific conversations with physicians about what's missing and why it matters.
For example, HCC documentation improvement is one area where that feedback loop pays off immediately. Providers need to capture chronic conditions with enough specificity every year to support accurate risk scoring, and autonomous coding can flag exactly where those details are missing at a granular level.
With that data in hand, organizations can show providers, "You're doing this X number of times, and it has X thousands of dollars of impact on your compensation." That kind of feedback changes charting behavior in ways that generic reminders to document more completely never have.
Future of CDI: From Manual Reviews to AI-Driven Revenue Integrity
For a long time, clinical documentation improvement lived in the compliance corner of the revenue cycle as a chart review function that was mostly reactive and manual.
Now, organizations are starting to treat clinical documentation improvement as central to how they protect revenue. Autonomous coding is a big part of this strategy. For the first time, CDI teams have visibility into the majority of charts, not just the small sample they can manually review.
As encounter volumes grow, organizations that invest in CDI as a core revenue cycle function will reduce denials, strengthen compliance, and ensure reimbursement reflects the care their teams provide. And for providers, better documentation means getting compensated for the work they're already doing.
If your organization is evaluating how clinical documentation improvement fits into a broader revenue integrity strategy, exploring what the right technology can do for your documentation quality is a good place to start.
Explore More Resources

Is Your Health System Ready for Autonomous Medical Coding? Five Questions to Ask

"Arintra is Doing the Heavy Lifting" Mercyhealth Transforms a Coding Capacity Challenge into Revenue Integrity at Scale

Med First Finds Its ‘Easy Button’ With Arintra: Over 6% Revenue Uplift, Stronger Compliance, and Reduced Provider Burden in One Solution

Mercyhealth boosts revenue by 5% and cuts aging days by over 50% while supporting accelerated growth

The Hidden Power of Coding in Transforming Revenue Cycle Management

Arintra Receives A+* Partnership Rating in KLAS Emerging Company Spotlight Report
Arintra’s Fully Automated Medical Coding Solution Now Available in Epic Toolbox

Mercyhealth Transforms Revenue Cycle Management With Arintra's Autonomous Coding Solution

Still on the fence about autonomous medical coding? Here’s what you’re missing
