Why Is Clinical Documentation Improvement Important? Because It's Where Revenue Problems Start



A denied claim or lower-than-expected physician compensation tend to send people looking at coding first. But follow the trail back far enough, and you usually end up in the same place: the documentation. A clinician charts a patient’s visit, but the note lacks the specificity required for accurate coding.
The claim either gets denied or paid at a lower rate than the care warranted. Nobody connects the dots until the pattern has been compounding for months, sometimes across hundreds of providers.
So why is clinical documentation improvement important? Because these patterns are fixable, but until recently, there hasn't been a practical way to address them at scale in high-volume settings.
The Two Levels Where Documentation Gaps Hurt
Documentation problems create financial consequences at two levels, and most organizations are only focused on one of them.
The organizational level
At the health system or physician group level, the impact of clinical documentation on reimbursement is direct: documentation quality determines how much revenue comes through the door for clinical services. The financial consequences play out in a few predictable ways:
- Denials: A Premier Inc. survey found that roughly 15% of claims face initial denial, with incomplete documentation driving a significant share of those rejections
- Rework costs: Each denied claim costs between $25 and $181 to rework and delays payment by weeks
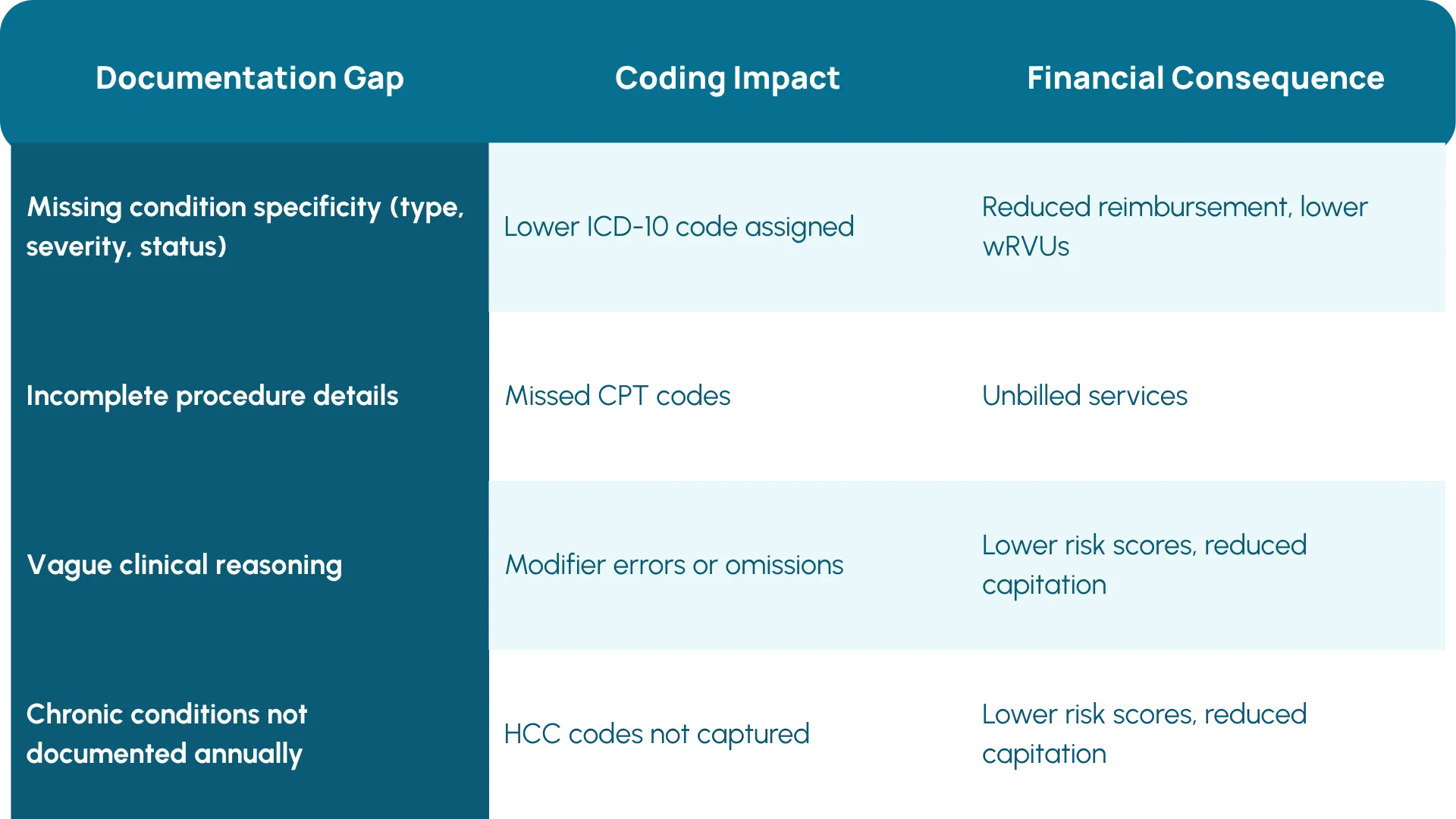
- Undercoding: Vague documentation forces coders or physicians to assign lower-level codes, which means organizations aren't reimbursed for the full complexity of care that their teams provided
These problems compound in outpatient settings, where encounter volumes are massive and most charts go to billing without a professional coder ever touching them. In many ambulatory settings, physicians code their own encounters.
The provider level
The organizational level is where most of these conversations usually stop, but they shouldn’t. Roughly 70% of physician compensation ties directly to work relative value units (wRVUs). Physicians see their wRVU numbers go up and down but rarely understand why, because nothing connects those changes back to specific encounters or documentation decisions.
A physician treats a complex diabetic patient but doesn't document the condition's type, control status, or complications. As a result, the documentation generates lower wRVUs for the care the physician delivered. Multiply that across hundreds of encounters, and the financial impact on a single provider can be significant.
The connection between charting habits and compensation is invisible to most physicians because nothing in their workflow makes it visible. And that connection turns out to be one of the most practical clinical documentation improvement benefits: providers who understand how documentation affects their compensation are more likely to change their behavior.
Why Traditional CDI Programs Haven't Solved This
If CDI in healthcare revenue matters this much, why aren't more organizations doing it well? The honest answer comes down to three things.
Traditional CDI was built for inpatient care
Individual inpatient claims are high enough in value to justify assigning a CDI specialist to review charts before they go to coding. You can pause the process, issue a query, and wait for the provider to respond.
Point-of-care alerts work against how physicians actually practice
Some vendors offer real-time documentation prompts that surface during the charting process. The idea makes sense in theory, but adoption in high-volume outpatient settings has been mixed. Physicians moving through 20 or 30 encounters a day tend to treat additional alerts as friction, and response rates often reflect that.
The inpatient model doesn't transfer to outpatient care
The volume is too high, the per-claim value is too low, and margins are too tight to support manual chart review at scale. An ACDIS survey found that nearly 73% of respondents either didn't have an outpatient CDI program or weren't aware of one at their organization. The reasons aren't hard to guess: cost, lack of clear ROI, difficulty scaling, and perhaps most fundamentally, no way to generate provider-level documentation data across charts at scale. You can't improve what you can't see.
What Changes When Autonomous Coding Enters the Picture
Something has changed about outpatient CDI, and that something is data. One main reason that clinical documentation improvement has been so hard to scale is that organizations couldn't tell you, at the provider level, which documentation habits were driving denials and costing money. Nobody was looking at all the charts, and until now, there wasn’t a way to.
Arintra’s autonomous coding platform makes this possible. By coding the majority of charts, the engine generates a detailed picture of documentation patterns at the provider, department, and organizational level. That data becomes the foundation for a completely different kind of documentation improvement, built on three principles:
- It's provider-specific, not generic. Instead of telling a physician "document more completely," you can show them: "You're omitting medication dosage changes on hypertensive patients, and across your encounters this year, that pattern has had a measurable impact on your compensation." As Med First CFO Wes Edwards put it, "When you give 50,000-foot advice, providers might not be able to change their charting behaviors. With Arintra, we're able to be very specific in our feedback to providers."
- It's retrospective, not interruptive. Feedback arrives after the encounter, based on the provider's own charts, tied to dollars they can see. It doesn't add steps to the documentation process or interrupt the provider's workflow.
- It gives providers time back. Providers whose charts are coded autonomously are no longer spending hours selecting codes. That time can go toward documenting with more specificity, or it can go back to patient care. Either way, it reduces the administrative friction that has historically made documentation improvement so hard to implement.
The Feedback Loop: Better Documentation, Better Coding, Better Revenue
Clinical documentation improvement in outpatient care is more viable right now than it's ever been, because autonomous coding creates a loop that didn't exist before:
- Autonomous coding processes the majority of charts, generating granular data on documentation patterns at the provider, department, and organizational level.
- Revenue cycle teams use that data to deliver targeted education to specific providers, support existing query workflows, or identify department-level trends.
- Providers adjust their documentation based on feedback tied to their own encounters and compensation.
- Better documentation produces more accurate codes, which reduces denials, increases reimbursement, and strengthens coding and compliance.
- As documentation improves, coding accuracy rises further, generating even more granular insights for the next round of education.
At Mercyhealth, this approach contributed to a 5.1% revenue uplift and a 50% reduction in A/R days. And the coding team, no longer buried under stacks of routine charts, now has the bandwidth to focus on provider education, compliance, denial analysis, and revenue integrity work.
What's Different About This Moment
Why is clinical documentation improvement important in outpatient care right now? The answer hasn't changed so much as the ability to act on it. Organizations have always known that documentation affects revenue. They just haven't had a way to fix it at scale.
Autonomous coding makes it possible to see outpatient documentation patterns at scale for the first time and to act on them in ways that change provider behavior. For health systems and physician groups trying to strengthen their revenue cycle, documentation improvement is the lever that makes everything else work better.
If your organization is exploring how to connect documentation improvement to coding and revenue outcomes in outpatient settings, a conversation about what autonomous coding can surface from your own data is a good place to start.
Learn how autonomous coding can help your organization improve coding accuracy, reduce compliance risk, and capture missed revenue.
Explore More Resources

Is Your Health System Ready for Autonomous Medical Coding? Five Questions to Ask

"Arintra is Doing the Heavy Lifting" Mercyhealth Transforms a Coding Capacity Challenge into Revenue Integrity at Scale

Med First Finds Its ‘Easy Button’ With Arintra: Over 6% Revenue Uplift, Stronger Compliance, and Reduced Provider Burden in One Solution

Mercyhealth boosts revenue by 5% and cuts aging days by over 50% while supporting accelerated growth

The Hidden Power of Coding in Transforming Revenue Cycle Management

Arintra Receives A+* Partnership Rating in KLAS Emerging Company Spotlight Report
Arintra’s Fully Automated Medical Coding Solution Now Available in Epic Toolbox

Mercyhealth Transforms Revenue Cycle Management With Arintra's Autonomous Coding Solution

Still on the fence about autonomous medical coding? Here’s what you’re missing
